



File photo of a 77th FS F-16CM.
Report Mentions Risks of Tactical Flying and Intense Training Demands, Wrong Decisions On The Ground Along with Possible Role of COVID-19 in Mishap.
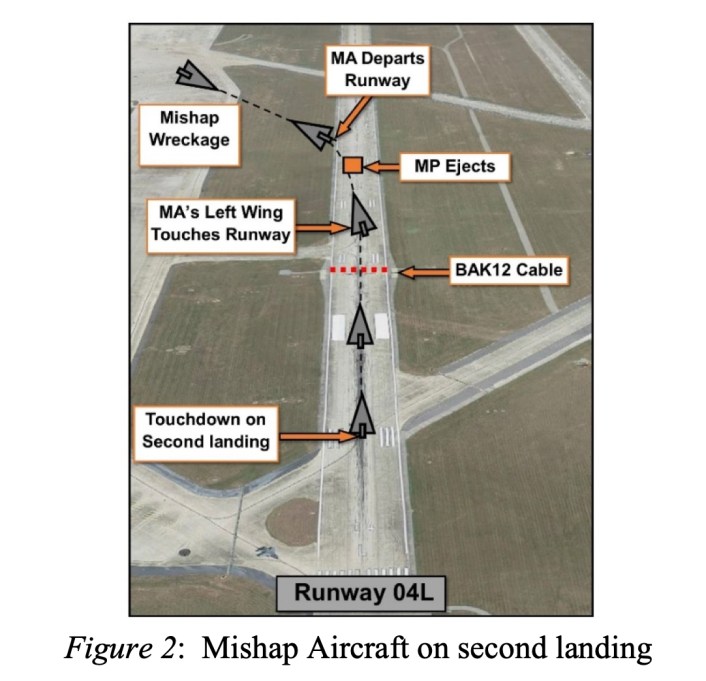
The cause of the tragic, fatal crash of an F-16CM, tail number 94-0043, assigned to the 77th Fighter Squadron, 20th Fighter Wing, on June 30, 2020 at Shaw AFB in South Carolina, that claimed the life of 1st Lt. David Schmitz, 32, originally of Santa Barbara, California, has been revealed in an official Air Force investigation released on November 9, 2020.“During the final phase of landing on runway 22R, the MA [Mishap Aircraft] struck the localizer antenna array short of the runway threshold, severely damaging the left main landing gear. After briefly touching down in the underrun, the MP [Mishap Pilot] executed a go-around and alerted the MEL and air traffic control personnel of the situation. Following more than twenty minutes of discussion between the supervisor of flying (SOF), the MEL, and MP it was decided to attempt an approach-end cable arrestment on runway 04L. During the maneuver, the MA’s tail hook did not catch the cable and the left wing fell to the runway, dragging the MA to the left. The MP ejected from the MA, but the ejection seat malfunctioned and the parachute did not deploy. The MP was fatally injured and the MA was destroyed.”

A file photo of USAF 1LT. David Schmitz, the F-16CM killed in the June 30, 2020 crash at Shaw AFB. (Photo: Facebook/via Laughlin AFB)
According to the formal accident report, USAF Maj. Gen. Randal K. Efferson, as President of the Accident Investigation Board, wrote that, “I find by a preponderance of evidence the cause of the mishap was the MP’s [Mishap Pilot’s] failure to correctly interpret the ALS [Automated Landing System] and identify the runway threshold during his first landing attempt, which resulted in severely damaged landing gear. Evidence also indicates the MP was not fully engaged on the challenges of flying a night instrument approach due to his unsuccessful attempt to conduct his first ever AAR [Air-to-Air Refueling] at night, which is not allowed by Air Force regulations. […] Two factors substantially contributed to the mishap: (a) the SOF chose not to consult the aircraft manufacturer, which resulted in the decision to attempt a cable arrestment in lieu of a controlled ejection and (b) a series of ejection seat malfunctions occurred, which resulted in the MP impacting the ground while still in the ejection seat.”
Human Factor.
The formal language of the report suggests the stressful and dangerous role of tactical combat pilots, and the exceptionally demanding nature of the nighttime midair refueling mission that 1LT. David Schmitz was assigned to the night of his fatal crash. 1LT. Schmitz had never attempted nighttime air-to-air refueling before the night of the accident.The report goes on to describe 1LT. David Schmitz as a competent, and in several ways, exceptional pilot. 1LT. Schmitz was selected as a Distinguished Graduate from his Undergraduate Pilot Training course and earned the Top Gun Award during Introduction to Fighter Fundamentals training, an “eight-week course designed to transform newly graduated pilots selected to fly fighters into fighter wingmen” according to the Air Force. The report also says that 1LT Schmitz was “lauded for his work ethic” and was graded as “slightly above average” in flying performance.
1LT. David Schmitz’s academic and flight training achievements are significant since, as with all military fighter branches, there is a saying that, “There are no average fighter pilots”. In order to qualify as a single-seat, tactical fighter pilot, officers must first pass through a long selection pipeline where fighter pilots are sorted from the top of flying performances and academic achievement in addition to personal conduct. 1LT. Schmitz was being graded as better than those already selected from being well above average.
The report evidences the high standards of performance that 1LT. Schmitz held himself to, and suggested he may have been frustrated (“distracted” according to the report language) by not being able to accomplish his first nighttime air-to-air refueling successfully.
On the return flight from the attempted midair refueling on the night of his fatal crash, 1LT. Schmitz’s element lead pilot, the pilot leading the flight, told 1LT. Schmitz over the radio that, due to flying conditions at the time, “That was not the way to start your tanking experience. That was really challenging”. But Schmitz was hard on himself for not accomplishing the tanker hook-up on the dark, turbulent night, replying to his flight leader over the radio, “No excuse”.
1LT. Schmitz had flown two training missions at night in the eight days before his fatal crash according to the accident investigation report.
According to the report, Schmitz was at current standards for night time landings and precision landing approaches. One paragraph of the report suggests the COVID-19 pandemic and its resultant quarantine and reduction in training may have been a contributing factor to the circumstances leading to the accident environment. According to the report, “The impact of the COVID mitigation measures is evidenced by the MP [Mishap Pilot] flying only two hours and two sorties from 60-90 days prior to the mishap”. However, 1LT. Schmitz’s flying hours in the eight days prior to the fatal accident may have partially moderated any potential erosion in proficiency or currency due to the reduced training tempo from the COVID-19 pandemic.
SOF decision
Dealing with the decision to attempt an arrested landing, here’s what in the report:“I believe the SOF’s decision to not call the aircraft manufacturer for technical assistance directly resulted in a decision to attempt an approach-end cable arrestment with less than favorable conditions in lieu of a controlled ejection. Specifically, the Air Force, in coordination with Lockheed Martin (LM), provides a dedicated hotline that an F-16 SOF, at any location around the world, can call for technical assistance when experiencing an in-flight emergency (IFE), which may not be specifically addressed in the pilot checklist. The program is known as the Conference Hotel (CH) procedure and was available at the time of the mishap. Following initial damage, the MA had more than thirty minutes of fuel remaining to troubleshoot the problem, so I assess there was time available to seek CH assistance. The critical items of the emergency were identified approximately six minutes after the initial damage occurred. The MA had a broken left main landing gear and system B hydraulic failure. Within two minutes, the SOF verbalized the two possible courses of action (COAs), which were to consider a controlled ejection or attempt an approach-end cable arrestment. The conditions that would favor one COA over the other COA were not discussed and the possibility of a controlled ejection was not mentioned again.”
“After the mishap, flight safety engineers from LM stated the mishap scenario did not match the Landing with Landing Gear Unsafe/Up checklist. The flight safety engineers explained that the pilot checklist for Unsafe/Up Landing Gear only applies if a landing gear fails to extend normally, and not when it is damaged or hanging. Had a CH been initiated, a LM flight safety engineer would have provided readily available information on two previous mishaps where F-16s experienced almost identical damage to the left main landing gear and associated hydraulic system. Both situations occurred in the daytime and resulted in a decision to execute a controlled ejection in lieu of attempting an approach-end cable arrestment. In both cases it was assessed that damaged and hanging landing gear could potentially interfere with or greatly reduce the chances of a successful cable engagement. Therefore, the LM flight safety engineers said that in this scenario it is unknown whether an F-16 with similar damage to the MA can safely engage an approach-end arresting cable.”
A graphic from the official Air Force accident investigation report of the fatal F-16CM crash on June 30, 2020 at Shaw AFB. (Photo: Official USAF Accident Report)
Ejection Seat
Dealing with the seat, “six of seven pyrotechnic devices in the seat should have activated during the MP’s ejection; however, the DRS [Digital Recovery Sequencer] failure resulted in none of them activating, and the subsequent failure of the stabilization gyro, trajectory divergence rocket motor, the harness release thruster, two drogue chute severance cutters, and primary parachute deployment cartridge. The failure of the DRS to initiate multiple devices resulted in the MP remaining in the MS and following a parabolic flight path until impacting the ground.Following a similar failure on a Tulsa F-16 in 2014 DRS a time compliance technical order (TCTO) 11P2-3- 502, Installation of the Shorting Plug on the DRS Electronic Module, was issued on Jan. 20, 2016. The shorting plug was designed to prevent noise bias issues observed in channel three of a three-channel system.
“Two channels are required to be in agreement for the DRS to function properly. Channel three noise bias issues have been observed in approximately 9% of all live ejections and sled tests. TCTO instructions allowed for installation of the shorting plug during regularly scheduled 36-month maintenance/inspections. Following issuance of the 2016 shorting plug TCTO [Technical Order] the first opportunity for installation on the MA was in August 2017. This was the regularly scheduled 36-month ejection seat maintenance/inspection, but TCTO shorting plug parts were not available, so the next installation date was moved three years to August 2020. In addition, the ten-year shelf/service life of the DRS installed in the MA expired in February 2019, but received three temporary service life extensions, extending it to 31 July 2020. All extensions were coordinated and approved by the Air Force Life Cycle Management Center. There was a small window of opportunity to replace the MA DRS in May 2020 with a newer system, which replaces the DRS and does not require a TCTO shorting plug. The newer system, known as the Modernized ACES II Seat Sequencer (MASS), became available in May 2020, but in order to consolidate maintenance actions, a request was granted to move the MASS installation to the July-August 2020 timeframe.”

Pilot Error And A Series of Ejection Seat Malfunctions Among The Causes Of Fatal F-16CM Crash at Shaw AFB.
Report Mentions Risks of Tactical Flying and Intense Training Demands, Wrong Decisions On The Ground Along with Possible Role of COVID-19 in Mishap. The
 theaviationist.com
theaviationist.com